
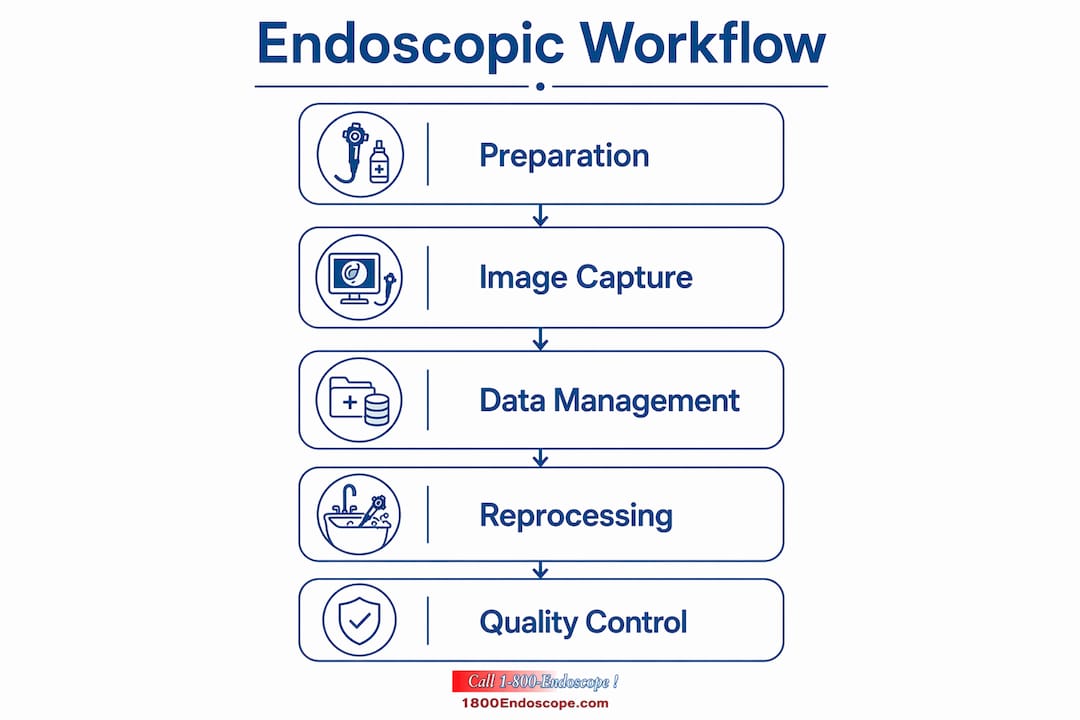
An endoscopic imaging workflow is the coordinated sequence of preparation, image acquisition, data management, and device reprocessing that produces accurate, repeatable diagnostic results. For veterinary clinics and industrial inspection teams, a poorly structured workflow means missed findings, contamination risk, and wasted procedure time. The 2026 standards from AAMI ST91 and the Joint Commission set clear benchmarks for every stage of this process. This guide covers the tools, steps, and best practices that keep your workflow consistent and compliant from the first scope check to the final data upload.
What are the essential tools for an endoscopic imaging workflow?
The right equipment determines what you can see and how reliably you can document it. Veterinary professionals work with rigid endoscopes for arthroscopy and cystoscopy, flexible gastroscopes for GI evaluation, and small diameter endoscopes for airway and nasal passages in small animals. Industrial technicians rely on borescopes and videoscopes to inspect turbine blades, pipelines, and engine cavities without disassembly.
Imaging technology has moved well beyond standard definition. HD white-light imaging is now the baseline for any professional setting. Image-enhanced endoscopy (IEE) techniques including Narrow Band Imaging (NBI), Linked Color Imaging (LCI), and Blue Light Imaging (BLI) add spectral contrast that highlights mucosal patterns invisible under white light. Standardized IEE classification systems show sensitivity as high as 98% in expert settings for early lesion detection. That level of accuracy depends entirely on having the right imaging modality matched to the clinical question.

Software integration closes the loop between image capture and documentation. PACS (Picture Archiving and Communication System), EMR/EHR platforms, and DICOM-compliant capture systems keep images tied to the correct patient or inspection record. DICOM-native systems prevent orphaned images and maintain record integrity as procedure volumes grow.
| Tool category | Key function |
|---|---|
| Rigid endoscopes | High-resolution imaging in fixed anatomical spaces |
| Flexible videoscopes | Navigation through curved lumens and GI tracts |
| Industrial borescopes | Remote visual inspection of enclosed mechanical systems |
| IEE imaging modules | Spectral contrast for mucosal and surface analysis |
| DICOM-compliant software | Automated image-to-record linking and audit readiness |
Pro Tip: Choose a light source matched to your imaging modality. Xenon and LED sources each have different spectral outputs that affect IEE performance. See the best light source guide for a direct comparison.
How to prepare and set up for an efficient endoscopic procedure
Preparation failures cause more procedure delays than equipment failures. A scope that arrives at the procedure room with a missed leak or residual debris forces an immediate halt, wastes sedation time, and creates infection risk. Pre-procedure inspection per 2026 best practices includes a visual check of the insertion tube, angulation controls, and all channels before the scope leaves the reprocessing area.
Room setup follows a fixed sequence. The processor, light source, monitor, and recording system must all be confirmed operational before the patient or inspection subject is positioned. For veterinary procedures, patient weight, species, and sedation protocol affect scope selection and insertion depth. For industrial jobs, access point diameter and cavity length determine which borescope diameter and working length you need.
A preparation checklist keeps every team member aligned:
- Confirm scope model matches the procedure requirements
- Verify leak test passed and documentation is logged
- Check all channel valves and biopsy port caps are seated
- Confirm light source output and monitor calibration
- Set recording system to the correct file format and storage destination
- Verify patient or inspection site is ready and accessible
Pro Tip: Run a white balance and color calibration check on your monitor at the start of each session. Color drift in aging monitors is a common source of misread mucosal patterns that goes unnoticed until image review.
Step-by-step execution for diagnostic accuracy
A standard diagnostic endoscopy procedure runs 6–10 minutes under optimal conditions. Every minute of that window needs to produce usable images. The execution phase breaks into five repeatable steps.
- Scope insertion and orientation. Advance the scope under direct visualization. Never force past resistance. Confirm anatomical landmarks before proceeding.
- Insufflation control. CO2 insufflation clears from the body up to 100 times faster than room air. Use CO2 for any procedure where post-procedure comfort and rapid recovery matter.
- Systematic image capture. Follow a defined mapping sequence so no region is skipped. In veterinary GI endoscopy, this means antrum, body, fundus, and retroflexion views documented in order.
- IEE activation for targeted areas. Switch to NBI, LCI, or BLI when a suspicious lesion or surface irregularity appears. Capture white-light and enhanced views of the same site for comparison.
- Image annotation and tagging. Label each image with location, modality, and any clinical observation before moving to the next site. Retroactive labeling during post-procedure review introduces errors.
The table below compares feature categories across imaging technique types:
| Imaging technique | Primary advantage | Best application |
|---|---|---|
| HD white-light | Broad overview, natural color | Routine survey and navigation |
| NBI | Vascular pattern contrast | Mucosal lesion characterization |
| LCI | Color differentiation of inflammation | Early mucosal change detection |
| BLI | Surface texture enhancement | Polyp margin definition |
Multimodal AI platforms that combine visual data with patient history match or exceed expert-level accuracy in lesion detection. These systems reduce operator dependency, which matters in veterinary and industrial settings where specialist availability is limited.
Pro Tip: For industrial borescope inspections, capture a reference image at the access point before advancing. This gives you a fixed orientation marker that prevents location confusion during report writing.
Best practices for reprocessing, data management, and workflow optimization
Reprocessing is where most workflow breakdowns occur. ANSI/AAMI ST91:2021 requires a minimum 10-minute dry time using pressure-controlled air after high-level disinfection. Skipping or shortening this step leaves residual moisture that supports microbial growth inside channels.
The physical layout of the reprocessing area matters as much as the protocol. A unidirectional workflow means soiled scopes enter one end of the reprocessing room and clean scopes exit the other, with no crossover between dirty and clean zones. Cross-pathing creates contamination risk even when manual cleaning steps are followed correctly.
Effective departments run reprocessing parallel to room turnover, not sequentially. Notification systems alert cleaning teams when a scope is incoming, so the next reprocessing cycle starts before the room is reset. This cuts turnaround time without cutting corners.
Common reprocessing and data management mistakes to avoid:
- Skipping the pre-clean flush immediately after scope withdrawal
- Using non-validated detergents that leave enzymatic residue
- Failing to log scope serial numbers against procedure records
- Storing scopes horizontally instead of vertically in drying cabinets
- Disconnecting image capture from EMR before the procedure record is closed
Automated image-to-record transfer eliminates the reconciliation risk that comes from manual data entry. AAMI ST91 and the Joint Commission require barcode or RFID tracking through every reprocessing step to prevent use of improperly processed devices.
Pro Tip: Assign one team member per session to own the data reconciliation step. Shared responsibility for image-to-record matching is the fastest path to orphaned files and audit failures.
How can emerging technologies and AI improve the endoscopic imaging workflow?
AI integration in endoscopy is past the proof-of-concept stage. Multimodal AI platforms that combine visual, textural, and patient-specific data now provide diagnostic support that reduces operator dependency in real time. For veterinary practices with limited specialist access, this changes what a general practitioner can reliably detect.
IEE technologies carry real clinical value, but the American Journal of Gastroenterology notes that their incremental benefit over HD white-light imaging is modest in many routine cases. The cost of IEE-capable systems must be weighed against the specific diagnostic goals of your practice or facility. Buying IEE capability for a workflow that rarely needs lesion characterization is a poor allocation of budget.
Key trends shaping advanced endoscopic workflows in 2026:
- AI-assisted polyp and lesion detection integrated directly into the imaging display
- Wireless videoscopes reducing cable management complexity in field inspections
- Cloud-based DICOM storage enabling remote image review and consultation
- Automated scope tracking dashboards replacing manual reprocessing logs
- Portable HD systems making specialist-quality imaging available in mobile veterinary units
The practical guidance here is to adopt technology in stages. Start with HD imaging and DICOM-compliant software. Add IEE capability when your case mix justifies it. Evaluate AI tools based on detection performance data, not marketing claims.
Key Takeaways
A structured endoscopic imaging workflow, built on AAMI ST91 standards, DICOM-compliant software, and unidirectional reprocessing, produces consistent diagnostic accuracy in both veterinary and industrial settings.
| Point | Details |
|---|---|
| Match tools to the task | Select scope type, diameter, and imaging modality based on the specific procedure and access requirements. |
| Preparation prevents delays | Complete a pre-procedure checklist covering scope integrity, equipment calibration, and site readiness before every session. |
| Unidirectional reprocessing is non-negotiable | Physical layout must separate soiled and clean zones to prevent cross-contamination regardless of protocol rigor. |
| Automate data transfer | DICOM-native software that links images directly to records eliminates reconciliation errors at scale. |
| Adopt AI in stages | Start with HD and compliant software, then add IEE or AI tools when your case volume and diagnostic needs justify the cost. |
What I've learned from building workflows across veterinary and industrial settings
The biggest mistake I see is treating reprocessing as a separate department problem. In practice, the imaging team and the reprocessing team share the same bottleneck. When image capture runs long because of poor scope navigation or missed documentation steps, the reprocessing queue backs up and room turnover stalls. The workflow is one system, not two.
Standardizing procedures across different environments is genuinely hard. A veterinary clinic running mixed species cases has different scope rotation needs than an industrial inspection team working a single facility. The answer is not one universal protocol. The answer is a modular checklist that covers the non-negotiable steps (leak test, dry time, DICOM tagging) and leaves room for site-specific adjustments.
Staff training is where most compliance gaps live. Technicians who understand why a unidirectional layout matters are far more likely to enforce it than those who follow a posted sign. Invest in training that explains the contamination mechanism, not just the rule. Audit trails only catch failures after the fact. Training prevents them.
The veterinary sterilization guide from 1800endoscope is one of the clearest resources I've seen for teams building or auditing their reprocessing protocols. It covers the steps that matter without padding.
— Endoscope
Equipment that supports a complete endoscopic imaging workflow
1800endoscope carries the equipment that covers every stage of the workflow described in this guide, from initial image capture to portable field inspection.
The veterinary rigid endoscopy catalog includes systems designed for small and large animal diagnostics, with HD video recording and compatible light sources. For industrial teams, the borescope and videoscope catalog covers portable options suited for confined-space inspections. 1800endoscope also stocks accessories including valves, biopsy forceps, and cleaning tools that keep your reprocessing workflow compliant. If you are building or upgrading a workflow, the full catalog at 1800endoscope.com is the right starting point.
FAQ
What is an endoscopic imaging workflow?
An endoscopic imaging workflow is the structured sequence of preparation, image capture, data documentation, and device reprocessing that produces accurate and repeatable diagnostic or inspection results. Every stage depends on the one before it.
How does AAMI ST91 affect reprocessing workflows?
AAMI ST91:2021 sets minimum standards for endoscope reprocessing, including a 10-minute pressure-controlled dry time and mandatory barcode or RFID tracking through every cleaning step. Non-compliance creates both patient safety risk and audit liability.
What imaging techniques improve diagnostic accuracy?
HD white-light imaging is the baseline standard. IEE techniques including NBI, LCI, and BLI add spectral contrast for lesion characterization, with NBI classification systems reaching sensitivity as high as 98% in expert settings.
How does AI fit into an endoscopic procedure workflow?
AI platforms that combine visual and patient data match expert-level lesion detection accuracy and reduce operator dependency. They are most valuable in settings where specialist availability is limited, such as mobile veterinary units or remote industrial sites.
Why does unidirectional layout matter in reprocessing?
A unidirectional physical layout keeps soiled and clean instruments on separate paths, preventing cross-contamination even when manual cleaning protocols are followed correctly. Cross-pathing is a contamination risk that protocol alone cannot eliminate.