
Sterilization in veterinary endoscopy is the process of eliminating all microbial life, including bacterial spores, from endoscopic instruments to prevent infection and protect patient safety during invasive procedures. Unlike high-level disinfection (HLD), which leaves a measurable residual microbial risk, sterilization achieves a Sterility Assurance Level (SAL) of 10⁻⁶, meaning no more than one in one million units carries a viable microorganism. Standards from ANSI/AAMI ST91 and guidance from SHEA (Society for Healthcare Epidemiology of America) both confirm that sterilization is preferred over HLD whenever the instrument and workflow allow. For veterinary clinics running flexible and rigid scopes across multiple procedures daily, getting this right is not optional.
How are veterinary endoscopes classified by risk?
The Spaulding classification system is the foundation for every endoscopic sterilization protocol in veterinary and human medicine. It divides devices into three categories based on their contact with body tissue.
- Critical devices contact sterile tissue or the vascular system. Rigid endoscopes used in arthroscopy, laparoscopy, or thoracoscopy fall here. These instruments require full sterilization before every use.
- Semi-critical devices contact mucous membranes or non-intact skin but do not penetrate sterile tissue. Flexible gastrointestinal endoscopes used in colonoscopy, gastroscopy, and bronchoscopy fall into this category. Flexible GI endoscopes require at least high-level disinfection, though sterilization is preferred when feasible.
- Non-critical devices contact only intact skin. These require low-level disinfection only.
The practical implication is direct: if you use a flexible endoscope to examine the esophagus of a dog, HLD is the minimum acceptable standard. If you use a rigid laparoscope to biopsy a liver, sterilization is mandatory. Misclassifying a device is one of the most common errors in veterinary practice, and it carries real infection risk.
Pro Tip: Post the Spaulding classification chart at every reprocessing station in your clinic. When staff can reference it without searching, protocol errors drop significantly.
The primary cause of endoscope-related infection outbreaks is the minimal safety margin of HLD compared to sterilization. That gap matters most in high-volume clinics where instruments cycle through multiple procedures in a single day.
Which sterilization methods work best for veterinary endoscopes?
Not all sterilization methods are compatible with all endoscope types. Choosing the wrong method damages instruments and creates false confidence in sterility.

| Method | Compatible Instruments | SAL | Key Limitation |
|---|---|---|---|
| Steam autoclave | Rigid endoscopes only | 10⁻⁶ | Destroys flexible endoscope components |
| Ethylene oxide (EtO) gas | Flexible and rigid | 10⁻⁶ | Long aeration time required |
| Hydrogen peroxide gas plasma | Most flexible endoscopes | 10⁻⁶ | Not suitable for long, narrow channels |
| High-level disinfection (HLD) | Flexible endoscopes | No SAL | Does not eliminate all spores |
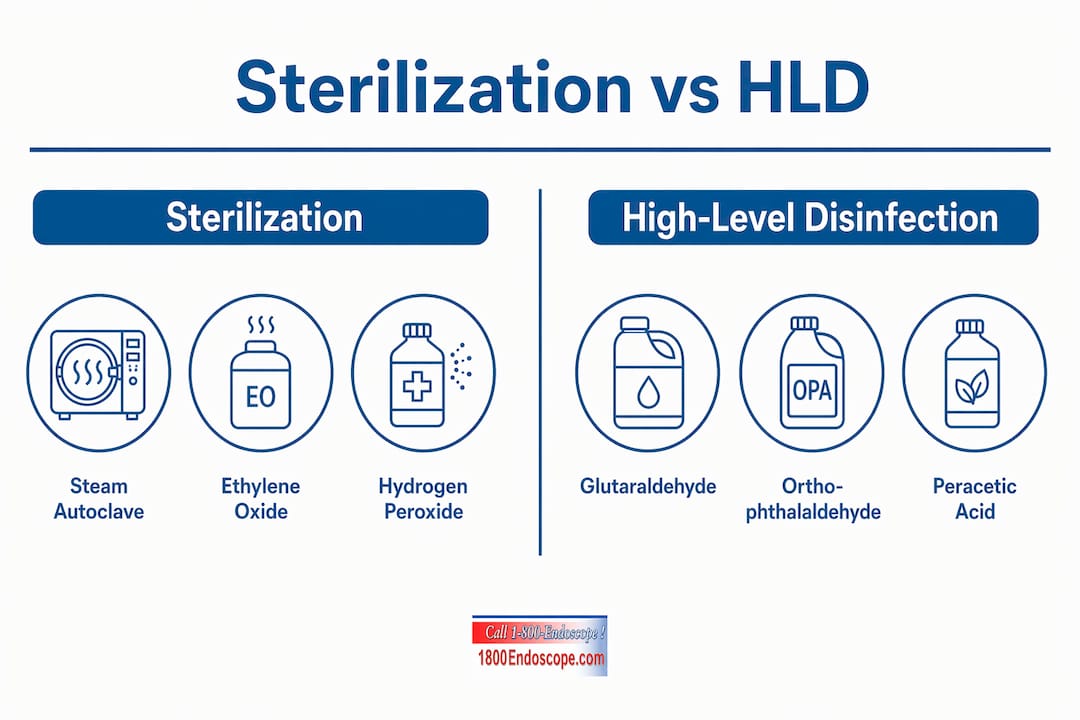
Steam autoclaving is appropriate for rigid endoscopes used in sterile body cavities but will warp or destroy the adhesives, lenses, and fiber bundles inside flexible scopes. Never autoclave a flexible endoscope.
Ethylene oxide sterilization is the only FDA-recommended method for flexible endoscopes that are difficult to sterilize by other means. EtO achieves a 10⁻⁶ SAL and eliminates multidrug-resistant organisms including MRSA, CRE, and E. coli. The trade-off is cycle time. EtO requires a full aeration period after sterilization, often 8–12 hours, to off-gas toxic residues before the instrument is safe to use. For clinics with high daily endoscope turnover, this means maintaining a larger instrument inventory or scheduling procedures accordingly.
Hydrogen peroxide gas plasma, used in systems like the STERRAD series, works well for most flexible endoscopes but has a critical limitation: it cannot penetrate channels shorter than a defined diameter or longer than a defined length. Always verify your specific endoscope model's compatibility before adopting this method.
High-level disinfection does not reliably eliminate all bacterial spores. That distinction matters when you are working with immunocompromised animals or performing procedures in contaminated tissue environments. HLD remains acceptable for semi-critical flexible endoscopes when sterilization is not feasible, but it should never be treated as equivalent to sterilization.
Pro Tip: Contact your endoscope manufacturer before selecting a sterilization method. Compatibility data is instrument-specific, and using an incompatible method voids warranties and may damage internal channels.
What does proper manual cleaning require before sterilization?
Manual cleaning is not a preliminary step. It is the step that determines whether sterilization will actually work. Sterilization does not clean instruments. Any organic debris remaining on or inside an endoscope will block sterilant penetration and leave viable microorganisms behind.
Follow this sequence for every flexible endoscope before sterilization or HLD:
- Wipe the insertion tube immediately after withdrawal from the patient using a soft, damp cloth to remove gross contamination before it dries.
- Perform leak testing before immersing the scope in any liquid. A single undetected perforation allows fluid ingress that destroys internal components.
- Flush all channels with enzymatic detergent solution using a syringe or channel flushing pump. Enzymatic cleaners break down protein-based debris that water alone cannot remove.
- Brush all accessible channels using the correct brush size for each channel diameter. Using wrong-size brushes fails to remove biofilm or may damage delicate channel walls. Match brush diameter to channel specifications from the manufacturer.
- Flush channels again after brushing to remove residual organic matter. Endoscope channels must be thoroughly flushed after brushing because residual debris can harbor biofilms that resist sterilization.
- Rinse with clean water and then purge channels with filtered air to remove moisture before sterilization.
Flexible endoscopes have long internal channels that cannot be visually inspected, which makes protocol adherence non-negotiable. You cannot see whether a channel is clean. You can only trust the process.
For rigid endoscopes going into an autoclave, the same principle applies. Instruments must be placed in an open position during sterilization. Closed ratchets and tightly stacked trays prevent steam from contacting all surfaces, which compromises sterility even when the cycle completes normally.
Pro Tip: Use a dedicated enzymatic detergent formulated for endoscopes, such as products meeting ASTM E1054 standards. General surgical instrument cleaners are not optimized for the channel geometry of flexible scopes.
How do you build and maintain sterilization protocol compliance?
Translating sterilization knowledge into consistent clinic practice requires written protocols, trained staff, and documented outcomes. Clinics that rely on verbal instruction and memory-based workflows produce inconsistent results.
Written protocols should align with ANSI/AAMI ST91, the primary U.S. standard for flexible endoscope reprocessing, and incorporate SHEA guidance where applicable. Update these documents annually or whenever you add new endoscope models to your inventory.
Staff training is not a one-time event. Every technician who handles endoscopes should complete structured training on cleaning, sterilization, and storage, with documented competency assessments. Turnover in veterinary clinics is high, and a new technician who skips a cleaning step creates the same infection risk as no protocol at all.
Key compliance elements to track and document include:
- Sterilization cycle logs with date, time, instrument ID, cycle parameters, and operator name
- Biological indicator (spore test) results, run at minimum weekly for each sterilizer
- Chemical indicator results from every sterilization pack
- Endoscope inspection records noting any damage, repairs, or channel irregularities
- Storage conditions, including hang time limits for scopes stored after HLD
Routine documentation, maintenance, and staff training are the structural backbone of infection control compliance. Traceability records also protect your clinic in the event of a post-procedure infection investigation.
Proper storage is the final link in the chain. Flexible endoscopes should be stored vertically in a ventilated cabinet, not coiled in a drawer. Coiling stresses internal components and traps moisture that promotes microbial growth. For small animal endoscopy settings, dedicated storage cabinets with HEPA-filtered airflow are the current best practice.
Key takeaways
Effective sterilization in veterinary endoscopy requires matching the correct method to the instrument type, completing thorough manual cleaning first, and maintaining documented compliance protocols aligned with ANSI/AAMI ST91 and SHEA standards.
| Point | Details |
|---|---|
| Sterilization vs. HLD | Sterilization achieves SAL 10⁻⁶; HLD does not eliminate all spores and carries measurable infection risk. |
| Spaulding classification | Rigid endoscopes require sterilization; flexible GI scopes require at minimum HLD, with sterilization preferred. |
| Method compatibility | Never autoclave flexible endoscopes; use ethylene oxide or hydrogen peroxide gas plasma instead. |
| Manual cleaning first | Organic debris blocks sterilant penetration; cleaning must precede every sterilization cycle. |
| Documentation and training | Cycle logs, spore tests, and competency records are required for infection control compliance. |
What i've learned after years of watching clinics get this wrong
The gap between written sterilization protocols and what actually happens at the reprocessing sink is wider than most clinic managers want to admit. I have seen well-equipped veterinary practices with current ANSI/AAMI ST91 binders on the shelf and technicians who have never read them. The binder does not protect the patient. The behavior does.
The most common failure point is not the sterilizer. It is the manual cleaning step. Clinics invest in EtO units or hydrogen peroxide plasma systems and then undermine the entire process by rushing the pre-cleaning phase. A scope that enters a sterilizer with residual protein debris will not come out sterile, regardless of how advanced the equipment is.
The second issue I see consistently is instrument compatibility confusion. Veterinary practices often acquire endoscopes from multiple sources over time, and nobody has verified which sterilization method each model can tolerate. That is how you end up with a warped flexible scope that was accidentally autoclaved, or a hydrogen peroxide plasma cycle run on a scope with channels too narrow for adequate gas penetration.
My honest recommendation: audit your reprocessing workflow before you audit your equipment. Observe a full cleaning and sterilization cycle from scope withdrawal to storage. You will find the gap. Then fix it with training, not just a new protocol document. The videoscope maintenance practices that protect instrument longevity are the same ones that protect your patients.
— Endoscope
Equip your clinic with endoscopes built for proper reprocessing
Choosing endoscopes that are compatible with validated sterilization methods is as important as the protocols themselves. 1800endoscope carries a full range of veterinary endoscopy systems designed for clinical use, including the portable 6mm airway endoscope suited for multi-procedure workflows where sterilization turnaround matters. For practices using rigid instruments, the veterinary rigid endoscopy catalog includes autoclave-compatible scopes built to withstand repeated sterilization cycles. Every system 1800endoscope offers is selected with real clinical workflows in mind, so you spend less time worrying about compatibility and more time on patient care.
FAQ
What is the difference between sterilization and high-level disinfection?
Sterilization eliminates all microbial life including spores and achieves a SAL of 10⁻⁶. High-level disinfection eliminates most microorganisms but does not reliably kill all bacterial spores, leaving a measurable residual risk.
Can flexible endoscopes be steam autoclaved?
No. Steam autoclaving destroys the adhesives, lenses, and internal channels of flexible endoscopes. Flexible scopes require low-temperature sterilization methods such as ethylene oxide or hydrogen peroxide gas plasma.
How often should biological indicators be used in veterinary sterilizers?
Biological indicators (spore tests) should be run at minimum once per week for each sterilizer in use, and with every load containing implantable devices. Results must be documented and retained for audit purposes.
Why does manual cleaning matter if the sterilizer kills everything?
Sterilization does not penetrate organic debris. Residual tissue, blood, or protein on instrument surfaces blocks sterilant contact and allows microorganisms to survive the cycle. Thorough manual cleaning is a prerequisite, not a backup step.
What standard governs flexible endoscope reprocessing in the u.s.?
ANSI/AAMI ST91 is the primary U.S. standard for flexible endoscope reprocessing. SHEA also publishes guidance that veterinary clinics should incorporate when developing or updating their sterilization protocols.