
Animal endoscopy is defined as the use of a thin, tube-like instrument equipped with a camera and light source to visually examine and treat internal organ conditions in animals without traditional open surgery. The industry standard term for this practice is veterinary endoscopy, and it covers both diagnostic and therapeutic applications across species ranging from cats and dogs to horses and exotic animals. The endoscope passes through natural body orifices or small incisions, transmitting real-time images to a monitor. General anesthesia or deep sedation is required for nearly all procedures. Flexible and rigid endoscopes are the two primary instrument categories, each suited to different anatomical targets and clinical goals.
What is animal endoscopy and why does it matter?
Veterinary endoscopy gives clinicians direct visual access to internal structures without the trauma of open surgery. The endoscope itself consists of a flexible or rigid tube, a high-resolution camera, a light source, and one or more working channels for instruments like biopsy forceps or snares. The camera transmits live video to a monitor, allowing the operator to navigate, assess tissue, and intervene in real time.
The clinical value extends well beyond visualization. Biopsy collection is one of the most important functions, providing targeted tissue samples that laboratory analysis can confirm or rule out disease with a level of accuracy that visual inspection alone cannot match. For cats presenting with chronic vomiting or weight loss, for example, endoscopic biopsy of the duodenum or ileum often reveals inflammatory bowel disease or alimentary lymphoma when radiographs appear normal.

Animal endoscopic surgery, the therapeutic arm of this discipline, extends the tool's role into active treatment. Foreign body retrieval, stricture dilation, and laser ablation are all performed through the working channel without a single external incision. That capability is what separates modern veterinary endoscopy from older diagnostic-only approaches.
What are the main types of veterinary endoscopy?
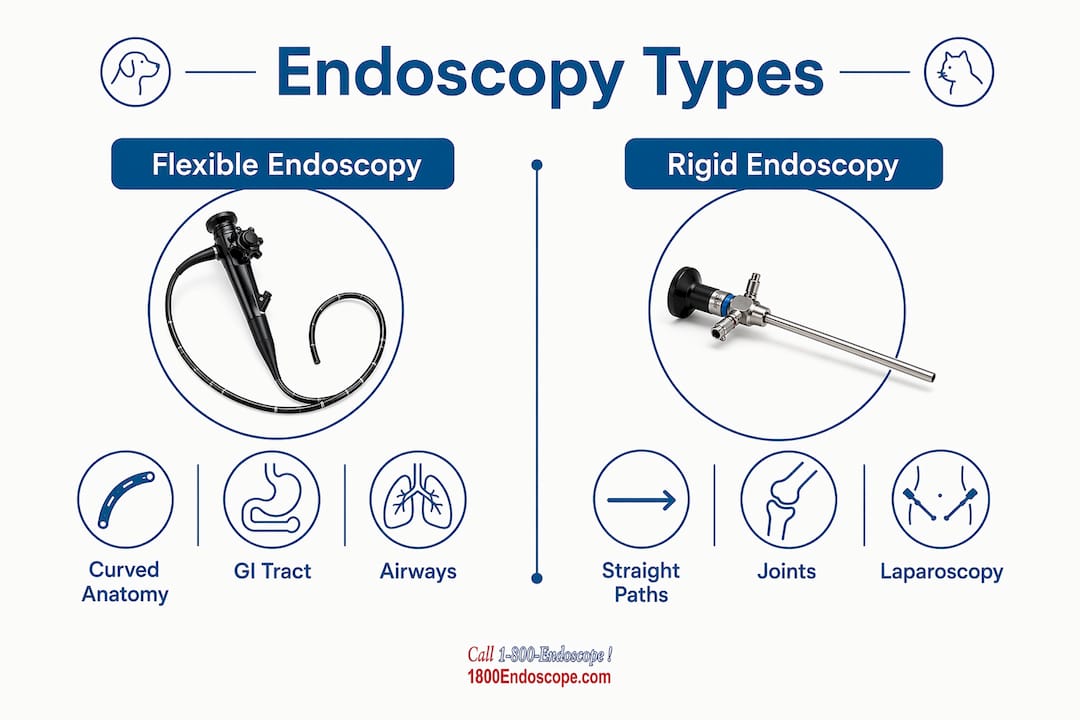
The two foundational categories are flexible endoscopy and rigid endoscopy. They differ in construction, target anatomy, and procedural technique.
Flexible endoscopes use a steerable, articulating tip that navigates curved luminal structures. Rigid endoscopes use a straight, fixed-angle tube suited to body cavities accessed through small portals.
| Feature | Flexible Endoscopy | Rigid Endoscopy |
|---|---|---|
| Primary targets | GI tract, airways, urinary tract | Joints, abdomen, nose, ears, thorax |
| Instrument flexibility | Fully articulating tip | Fixed angle, straight shaft |
| Key advantage | Navigates curved anatomy | Superior optics, larger working channel |
| Main limitation | Fragile; requires careful handling | Cannot access curved luminal structures |
| Common procedures | Gastroscopy, colonoscopy, bronchoscopy | Laparoscopy, rhinoscopy, arthroscopy |
Flexible endoscopes are primarily used for examining the esophagus, stomach, small intestines, colon, urinary tract, and trachea. Rigid endoscopes are the instrument of choice for joints, abdominal exploration, nasal passages, ear canals, and the thoracic cavity. Choosing the wrong type for a given case is a common early-career mistake that compromises both image quality and procedural safety.
Specialized subtypes include laparoscopy, which uses rigid portals and carbon dioxide insufflation to examine the abdominal cavity, and thoracoscopy, which applies the same principle to the chest. Both require additional training beyond standard flexible endoscopy.
Pro Tip: When selecting a scope for small patients like cats or toy breeds, small diameter endoscopes in the 5–8 mm range reduce mucosal trauma and improve maneuverability in tight anatomical spaces.
How is an animal endoscopy procedure performed?
A structured procedural workflow determines both safety and diagnostic yield. Skipping steps in preparation is the most common source of avoidable complications.
- Pre-procedure workup. Bloodwork and physical exam are required before every endoscopic procedure to assess anesthetic risk and confirm patient suitability. Coagulation status matters especially when biopsy is planned.
- Fasting and bowel preparation. Upper GI endoscopy requires 12–18 hours of fasting. Colonoscopy requires complete colonic evacuation using oral lavage solutions or enemas, since retained fecal material blocks visualization entirely.
- Anesthesia induction. General anesthesia is standard. Propofol induction followed by isoflurane maintenance is a common protocol. Endotracheal intubation protects the airway during upper GI procedures.
- Room and equipment setup. Procedure rooms are optimized with dimmed lighting and monitor positioning that allows the operator to look directly at the screen without turning away from the patient. For laparoscopy, an insufflator delivers carbon dioxide to distend the abdominal cavity and create working space.
- Scope insertion and navigation. The endoscope enters through the appropriate orifice or portal. The operator advances under direct vision, using air or water insufflation to open luminal structures and improve visualization.
- Diagnostic and therapeutic steps. Tissue sampling uses biopsy forceps passed through the working channel. Foreign bodies are grasped with retrieval forceps or basket snares. Strictures are dilated with balloon catheters.
- Recovery and monitoring. Most patients are discharged the same day. Post-procedure monitoring focuses on anesthetic recovery, pain scoring, and signs of complications such as abdominal distension or respiratory distress.
Pro Tip: Light source quality directly affects image resolution and diagnostic accuracy. Reviewing light source selection before purchasing or upgrading equipment prevents a common bottleneck in image quality that no camera upgrade can fix.
What are the diagnostic and therapeutic applications?
The benefits of animal endoscopy are clearest when you compare outcomes to the alternative: open surgery or empirical treatment without tissue diagnosis.
Diagnostic applications include:
- Gastrointestinal disorders: chronic vomiting, diarrhea, weight loss, protein-losing enteropathy, and suspected neoplasia
- Respiratory tract evaluation: chronic cough, nasal discharge, epistaxis, and suspected tracheal or bronchial lesions
- Urinary tract examination: hematuria, recurrent urinary tract infections, and suspected bladder masses
- Detection of foreign bodies, mucosal inflammation, ulceration, polyps, and intraluminal masses
- Targeted tissue biopsy for histopathology, culture, and cytology
Therapeutic applications include:
- Foreign body removal, stenting, laser therapy, and stricture dilation, all performed through the working channel without open incision
- Polypectomy and mass debulking in the GI tract and bladder
- Nasal flushing and rhinoscopic debridement in chronic rhinitis cases
- Laparoscopic ovariectomy and cryptorchid castration in dogs and cats
The cat endoscopy diagnostic benefits are particularly significant in feline medicine, where chronic enteropathy is common and tissue diagnosis changes treatment protocols substantially. A cat with suspected inflammatory bowel disease versus low-grade intestinal T-cell lymphoma requires completely different management, and endoscopic biopsy is the tool that makes that distinction possible without exploratory laparotomy.
Veterinary specialists confirm that therapeutic endoscopy significantly reduces patient recovery times compared to open surgeries. A dog recovering from endoscopic foreign body removal is typically eating within hours. The same dog recovering from a gastrotomy needs 10–14 days of restricted activity and wound management.
What are the risks and limitations of animal endoscopy?
Endoscopy is minimally invasive, not risk-free. Every practitioner performing these procedures needs a clear-eyed understanding of where the technique can fail.
Key risks include:
- Anesthesia complications, which represent the most common source of morbidity, particularly in geriatric or systemically ill patients
- Organ wall perforation, which is rare but serious; the risk increases with aggressive biopsy technique, friable tissue, or operator inexperience
- Infection from inadequately reprocessed instruments; strict cleaning protocols for biopsy forceps, snares, and scope channels are non-negotiable for preventing cross-patient contamination
- Respiratory compromise during upper airway or esophageal procedures, especially in brachycephalic breeds
Limitations that affect case selection:
- Patient size: very small patients (under 2 kg) may not tolerate standard scope diameters
- Tumor size and location: large intraluminal masses or lesions in anatomically inaccessible areas may require open surgery
- Operator skill: the steep learning curve for veterinary endoscopy directly impacts procedural safety and duration; case outcomes improve significantly with operator experience
Careful patient selection is paramount, as anatomical and tumor size limitations can preclude safe endoscopic approaches. Every endoscopic procedure should begin with a documented plan for conversion to open surgery if the endoscopic approach fails or reveals a condition beyond its scope.
Endoscopy is a decision-making tool as much as a procedural one. The decision to proceed, modify, or convert to open surgery requires the same clinical judgment as any other surgical choice.
The case for building endoscopy into your practice
Veterinary endoscopy is not a specialty-only skill set anymore. General practitioners who invest in training and equipment are delivering faster diagnoses, fewer exploratory surgeries, and measurably better recovery outcomes for their patients.
The equipment acquisition question is real. Quality flexible videoscopes and rigid laparoscopy systems represent significant capital investment. What I have seen consistently, though, is that practices treating endoscopy as a cost center rather than a revenue-generating diagnostic service underutilize the equipment and undervalue the clinical returns. A single endoscopic foreign body retrieval that avoids a gastrotomy pays for a significant portion of a portable system.
The therapeutic applications are where the discipline is heading. Laparoscopy and thoracoscopy are no longer fringe techniques. Board-certified surgeons at referral centers perform them routinely, and the gap between referral-level and general practice capability is narrowing as training programs and affordable equipment improve. Practices that build endoscopy competency now will be positioned ahead of that curve.
Patient selection discipline matters more than equipment. The most common errors I observe are attempting endoscopy on patients with inadequate bowel preparation, proceeding without a clear conversion plan, and underestimating anesthetic risk in compromised patients. Get those fundamentals right before worrying about scope diameter or camera resolution.
For small animal endoscopy tips grounded in real clinical scenarios, the practical guidance available for veterinary professionals covers the procedural details that textbooks often skip.
— Endoscope
Veterinary endoscopes and systems from 1800endoscope
1800endoscope stocks a full range of veterinary endoscopic systems built for clinical use, from portable flexible videoscopes to rigid laparoscopy setups and equine airway scopes.
The portable 6mm airway system is a practical starting point for clinics adding flexible endoscopy to their diagnostic toolkit. It includes a direct monitor, SD card video recording, and a compact form factor suited to both small animal and equine airway work. For practices focused on gastric and lower GI applications, the economy gastroscope delivers a 10mm working diameter at 3 meters, covering the full upper GI tract in dogs and large cats. 1800endoscope also carries light sources, biopsy forceps, valves, and cleaning accessories. Browse the full veterinary catalog or visit the FAQ page for equipment guidance.
Key takeaways
Veterinary endoscopy delivers accurate diagnosis and minimally invasive treatment through direct visualization, targeted biopsy, and working-channel intervention, making it one of the most clinically versatile tools in modern animal medicine.
| Point | Details |
|---|---|
| Two core instrument types | Flexible scopes target luminal structures; rigid scopes access joints, abdomen, and thorax. |
| Anesthesia is required | Every endoscopic procedure needs pre-procedure bloodwork and general anesthesia or deep sedation. |
| Biopsy drives diagnosis | Targeted tissue sampling through the working channel provides histopathology that imaging cannot replace. |
| Therapeutic range is broad | Foreign body removal, stricture dilation, laser therapy, and laparoscopic surgery all fall within endoscopic capability. |
| Instrument reprocessing is critical | Strict cleaning and maintenance protocols for all endoscopic tools prevent cross-patient contamination. |
FAQ
What is animal endoscopy used to diagnose?
Veterinary endoscopy diagnoses GI disorders, respiratory tract lesions, urinary tract abnormalities, foreign bodies, and internal masses through direct visualization and targeted biopsy. It is particularly valuable when imaging findings are inconclusive and tissue diagnosis is needed.
How much does a veterinary endoscopy procedure cost?
Veterinary endoscopic procedures typically cost $800–$3,000, depending on the procedure type, patient size, and whether therapeutic intervention is performed alongside diagnosis.
What is the difference between flexible and rigid endoscopy?
Flexible endoscopy navigates curved luminal structures like the GI tract and airways, while rigid endoscopy accesses joints, the abdominal cavity, nasal passages, and the thorax through small portals. The choice depends entirely on the target anatomy.
Is animal endoscopy safe?
Endoscopy is generally safe when performed by trained operators on appropriately selected patients. The main risks are anesthesia complications and, rarely, organ perforation. Operator skill and patient selection are the two variables that most directly influence safety outcomes.
How long does recovery take after veterinary endoscopy?
Most patients are discharged the same day and return to normal activity within 24–48 hours. Recovery is significantly faster than open surgery, which is one of the primary clinical benefits of endoscopy for animals.